
You’ve watched the therapy appointments stack up. You’ve tracked the medication changes, the dose adjustments, the switches to something new. You’ve sat through panic attacks and sleepless nights and days when leaving the house felt impossible. You’ve done everything right, and it hasn’t been enough.
If you’re searching for anxiety help for someone you love and wondering whether residential treatment is the next step, that search itself is telling you something. Severe anxiety that hasn’t responded to outpatient care is a clinical problem, and it deserves a clinical answer instead of another round of wait and see.
If you’re not sure whether what you’re seeing rises to the level of residential care, a confidential conversation with the clinical team at Destination Hope can help you understand your options for care.
What this article covers
- How to tell when anxiety has moved past what outpatient therapy and medication can reach.
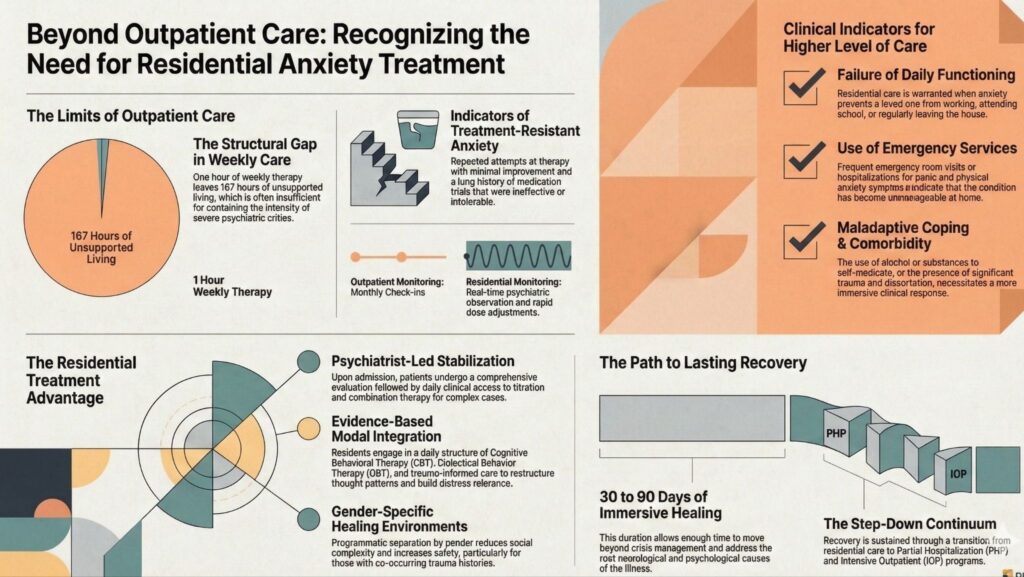
- What residential mental health treatment provides that weekly appointments can’t: psychiatrist-led stabilization, daily therapy, and around-the-clock clinical support.
- Why choosing this level of care for a loved one with severe anxiety is a clinically appropriate response, not an overreaction.
- How a full continuum of care, with PHP and IOP step-downs, supports the work after a residential stay ends.
When Anxiety Becomes More Than Outpatient Care Can Handle
The Difference Between Manageable Anxiety and a Psychiatric Crisis
Anxiety runs along a spectrum. At one end is the ordinary tension before a hard conversation or a brutal week at work. At the other end is a psychiatric condition that has dismantled a person’s ability to function.
Generalized anxiety disorder, panic disorder, social anxiety disorder, and related conditions are real illnesses with neurological and psychological roots. For many people they respond well to outpatient treatment: a good therapist, the right medication, steady support. For others, the illness is more severe, more treatment-resistant, or more tangled up with trauma, co-occurring conditions, or biological factors that one weekly hour can’t reach.
The difference comes down to acuity, and acuity determines what level of care actually fits. It has nothing to do with willpower or effort.
When anxiety has reached the point where your loved one can’t work, can’t hold relationships together, can’t manage basic daily functioning, or is having physical symptoms severe enough to land them in the emergency room, that is a psychiatric crisis. It belongs in a psychiatric setting, not on a waitlist for an outpatient slot.
Signs Your Loved One’s Anxiety Has Crossed a Clinical Threshold
Use this as a quick self-check. If several of these describe your loved one’s situation, residential treatment is worth a serious conversation.
- Outpatient therapy has continued for months or years without meaningful improvement.
- They’ve tried two or more medications without adequate relief.
- Anxiety is keeping them from working, attending school, or leaving the house regularly.
- There have been emergency room visits or hospitalizations tied to panic or anxiety symptoms.
- The anxiety comes with significant depression, dissociation, or trauma-related symptoms.
- They’re using alcohol or other substances to manage anxiety symptoms.
- You, as a family member, are reorganizing your own life around their anxiety to help them cope.
If you said yes to three or more, what you’re describing isn’t mild anxiety that needs a better coping toolkit. It’s a condition that has become unmanageable, and it deserves care at the matching level of intensity. The Cleveland Clinic notes that untreated anxiety disorders can lead to complications including alcohol and substance use disorders, which is one reason a thorough evaluation matters when anxiety has gone this long without relief.
Why Standard Treatment Often Falls Short for Severe Anxiety
The Limits of Weekly Therapy and Medication Management Alone
Outpatient care is built for a certain range of severity. A weekly therapy session gives someone tools to practice, room to process, and a steady therapeutic relationship. For many people with anxiety, that’s enough.
For others it isn’t. That’s a structural limitation, and it says nothing about how hard the person or the therapist is working. One hour a week, with 167 hours of unsupported living in between, can’t provide the containment that severe anxiety requires. Medication management in an outpatient setting often means a monthly check-in at best, with little ability to watch response closely, adjust quickly, or untangle the psychiatric complexity that frequently sits underneath treatment-resistant anxiety.
When anxiety is rooted in complex trauma, co-occurs with other mood or thought disorders, or has become so entrenched that the nervous system stays stuck in chronic activation, the standard outpatient model doesn’t have the tools to break that cycle.
What Treatment-Resistant Anxiety Actually Looks Like
Treatment-resistant anxiety isn’t a separate diagnosis. It’s a pattern: repeated trials of appropriate treatment that haven’t produced the improvement a person’s functioning requires. It’s also more common than most families realize. A review in the Mental Health Clinician reports that around half of patients treated for generalized anxiety disorder fail to respond to their initial treatment.
In practice, it looks like someone who has seen three therapists and found each helpful to a point, never past it. Sometimes it’s a medication history that spans a decade, full of trials that either didn’t work or couldn’t be tolerated. Often it’s a person who has picked up secondary problems along the way, like social isolation, substance use, depression, or declining physical health, because the underlying anxiety was never treated adequately.
Families living with treatment-resistant anxiety often describe a specific kind of exhaustion. They know their loved one is trying. They know the outpatient providers are trying. And still nothing shifts. That exhaustion is a signal worth listening to. It’s the system telling you the current level of care isn’t matched to the clinical need.
You’ve done everything outpatient care could offer. There’s a next step, and it doesn’t have to look like a hospital.
What Residential Mental Health Treatment Offers That Outpatient Cannot
Psychiatrist-Led Stabilization and Medication Evaluation
In a residential mental health setting, the psychiatric work happens in real time. A psychiatrist isn’t reviewing a month of symptom logs during a 20-minute appointment. The clinical team observes your loved one daily, adjusts treatment as the picture changes, and works from how that person is actually functioning, day to day, well past what a single Tuesday check-in can capture.
For people with severe anxiety, that access matters. Medication management for complex anxiety often calls for careful titration, combination approaches, and attention to how anxiety interacts with sleep, nutrition, trauma symptoms, and any co-occurring conditions. That kind of precision is realistic only in an environment where the team has daily contact and can respond quickly.
At Destination Hope, our psychiatrist-led team completes a comprehensive evaluation on admission, then builds an individualized treatment plan that addresses the full clinical picture. We don’t treat anxiety as a standalone problem to be quieted. We look at what else is present, what’s already been tried, and what the neurological and psychological roots of the illness actually are.
Immersive, Evidence-Based Therapy: CBT, DBT, and Trauma-Informed Care
Residential treatment replaces one weekly hour with a structured environment where the healing work becomes the daily architecture of life.
Cognitive behavioral therapy is the most common psychotherapy used for anxiety disorders, according to the Cleveland Clinic, with strong evidence for restructuring the thought patterns that keep anxious responses running. Dialectical behavior therapy builds the distress-tolerance and emotional-regulation skills that help people manage acute symptoms and form a different relationship with their internal experience. Trauma-informed care addresses what often sits underneath: adverse experiences, attachment disruption, and chronic stress responses the nervous system was never given the resources to resolve.
In a residential setting these approaches don’t run in isolation. They’re woven into a daily structure of individual therapy, group work, skill-building sessions, nutrition programming, and psychiatric oversight, so progress can consolidate from one day to the next instead of fading between appointments.
Getting Anxiety Help for a Loved One in South Florida
What to Expect From the Admissions and Evaluation Process
Calling an admissions team when your loved one is in crisis, or when you can’t tell whether their situation even qualifies, can feel like a high-stakes leap. It doesn’t have to.
At Destination Hope, the admissions process begins with a clinical conversation. No sales pitch. Our team asks about your loved one’s history, current symptoms, prior treatment, and what hasn’t worked. The aim is an honest clinical read: whether residential care is the right level, and whether Destination Hope is the right fit for what your loved one needs.
If residential care fits, we’ll walk you through what to expect: the comprehensive psychiatric evaluation at intake, the individualized treatment plan, and the rhythm of daily life at our facility in Tamarac, in Broward County. If it isn’t the right fit, we’ll tell you, and point you toward what might be.
How Gender-Specific Residential Care Creates Conditions for Real Progress
The treatment environment shapes the outcomes. Destination Hope provides gender-specific residential programming because many people with severe anxiety, especially those carrying co-occurring trauma histories, do more meaningful clinical work in a setting where they feel safe and where group therapy doesn’t carry the added social complexity of a mixed-gender room.
Residential stays of 30 to 90 days give people enough time to do the deeper work: understanding the root causes of the anxiety, building the skills to manage it, and establishing a new baseline for functioning. Our step-down continuum, including a Partial Hospitalization Program, an Intensive Outpatient Program, and extended care, gives the progress made in residential treatment a foundation to keep building on after discharge.
Frequently Asked Questions
How do I know if my loved one’s anxiety is severe enough for residential treatment?
If outpatient therapy and medication management haven’t produced meaningful improvement over months or years, if anxiety is keeping your loved one from working or managing basic functioning, or if there have been hospitalizations or emergency interventions, the severity likely warrants a higher level of care. A clinical consultation can help you assess it directly.
What’s the difference between residential mental health treatment and a psychiatric hospital?
A psychiatric hospital focuses on acute stabilization, getting someone safe enough to discharge, usually within days. Residential treatment offers weeks or months of intensive psychiatric care, therapy, and skill-building in a dignified, structured environment. The goal there reaches past safety to genuine clinical progress.
Can anxiety disorders be treated in a residential setting without a substance use issue?
Yes. Destination Hope provides primary psychiatric residential care for anxiety disorders and other mental health conditions. Substance use doesn’t need to be present. When it is, it’s treated at the same time as a co-occurring condition.
What does a typical day look like in a residential anxiety treatment program?
Days are built around individual therapy, group sessions, psychiatric appointments, medication management, skill-building, nutrition support, and unstructured time for rest and integration. For people with severe anxiety, that structure is itself therapeutic.
How long does residential treatment for severe anxiety usually last?
Stays at Destination Hope run from 30 to 90 days, depending on clinical need and progress. Length is set by the treatment team in collaboration with the individual and their family.
Will my loved one’s insurance cover residential mental health treatment for anxiety?
Destination Hope accepts most major insurance plans. Our admissions team can verify insurance and payment details and walk you through coverage before you make any decisions.
How do I talk to someone I love about getting more intensive help for their anxiety?
Lead with what you’ve observed instead of what you think they should do. “I’ve watched how much you’re struggling, and I want to find something that actually helps” lands differently than “you need to go somewhere.” Our family team can also consult with you on how to approach these conversations.
What happens after residential treatment? Is there ongoing care?
Destination Hope provides a full continuum of care. Most residents step down to our PHP or IOP programs for continued intensive support while transitioning back to daily life. Continuing care planning starts early in the residential stay, not as an afterthought at discharge.
Talk to Someone Who Has Seen This Before
You don’t have to figure this out alone. If your loved one has been living with severe anxiety and outpatient care hasn’t been enough, reach out. We’ll help you understand whether residential treatment is the right fit and what the path forward could look like. Call our admissions team at (954) 302-4269 or start a confidential inquiry.
Crisis and Emergency Resources
If you or someone you know is in a substance use or mental health crisis, help is available now. Contact the SAMHSA National Helpline at 1-800-662-HELP (4357) for free, confidential treatment referrals 24/7. Reach the 988 Suicide and Crisis Lifeline by calling or texting 988. The Crisis Text Line is available by texting HOME to 741741. For emergencies, call 911.





